


A Word About Murmurs...
An interesting case with KEY lessons

We’ve been in the clinical education space for quite some time, and murmurs are always a challenge for both students and clinicians. Recently, in our WhatsApp group, we had a discussion on differentiating murmurs, with some clinicians sharing useful ways to differentiate murmurs. (Email us at info@paretoeducation.co.uk if you’d like to join.)

I got a real taste of “murmur action” recently with a patient who booked into my clinical in general practice. He was in his late 30s, worked in a warehouse, didn’t smoke, and drank occasionally. His main complaint was palpitations.
Palpitations is usually bread and butter stuff. Examine the patient, rule out atrial fibrillation and request some bloods (including thyroid function tests) and an ECG. Normally these results are normal which is unsurprising as an ECG is really a “picture” of the heart over 10 seconds. Typically, we refer such patients for a 24-hour heart monitor.
This case, however, was different. The patient was noticeably short of breath and visibly uncomfortable. Could this be supraventricular tachycardia (SVT)? Or perhaps an atrial tachycardia, which occasionally requires A&E intervention? I’ve seen many cases like this, but something about this man stood out—he was REALLY uncomfortable.
He was clammy, short of breath, and pale. I asked if he had chest pain, but he denied it—just palpitations for the past two days. There was no clear trigger, as he denied excess alcohol, fever, diarrhea, or any other symptoms.
I felt his pulse—it was fast, really fast, but regular. His heart rate was around 135 beats per minute, yet his blood pressure was stable at 135/89. On chest examination, his lungs sounded clear at first, but when I listened more closely, I could hear bilateral crackles at the lung bases.
“Have you had any leg swelling?” I asked,
“No, none at all.”
Yup.. I was thinking heart failure. This was unusual for someone so young. Then, when I listened to his heart, I heard one of the loudest murmurs I've ever encountered.
To simplify murmur assessment in adults, I typically focus on two main types:
Ejection systolic murmurs (ESM)
Sound: Crescendo-decrescendo (diamond-shaped), heard best during systole.
Cause: Due to turbulent blood flow across a narrowed or obstructed outflow tract (e.g., aortic stenosis, pulmonary stenosis).
Pan-systolic murmurs (PSM)
Sound: Uniform, high-pitched, "blowing" murmur that lasts throughout systole.
Cause: Due to abnormal blood flow from a high-pressure to a low-pressure chamber (e.g., mitral regurgitation, tricuspid regurgitation, ventricular septal defect).
Picture demonstrating the position of murmurs

This patient had a pan-systolic murmur, which is usually loudest at the mitral valve area. However, this murmur was loud everywhere, which was highly unusual. Normally, such widespread intensity is seen with ejection systolic murmurs, but in this case, the murmur persisted throughout systole (cardiac contraction).

Then, there was another key finding. When I placed my stethoscope on his chest, I felt a distinct rumbling. It was strong… it was a loud. Almost like an earthquake contained within the palm of my hand. Clinical practice often involves linking sensory observations with prior knowledge, and deep in my memory, I recalled something about heaves.
A heave is a forceful, sustained movement of the chest wall, often due to ventricular hypertrophy, which signals increased cardiac workload.
A left parasternal heave suggests right ventricular hypertrophy (e.g., pulmonary hypertension).
An apical heave indicates left ventricular hypertrophy (e.g., aortic stenosis, hypertension).
This patient's heave was strong, creating a distinct rumbling against my hand—a clear sign of significant cardiac pathology.
So I decided to have this man admitted. There was no time to wait and a member of his family was with him so I had him sent across to A&E. I sent him with a letter that said something like:
Dear colleague,
This is MR XYZ who presented with a 2 day hx of palpitations. He is significantly short of breath and my examination finds him to have a pan systolic murmur with cardiac thrills. His HR is 135 and his blood pressure is stable. I would appreciate it if you could review this gentleman,
Kind regards
Dr M
I thought about him for a while but as you do in general practice, you move onto the next customer.. I mean patient. Some coughs and colds, mental health reviews, shoulder pains were to follow as well as a long list of admin tasks. Towards the end of the day, I received a message from a clinician who I hadn’t spoken to in some years. It was a colleague of mine who I worked with in A&E:
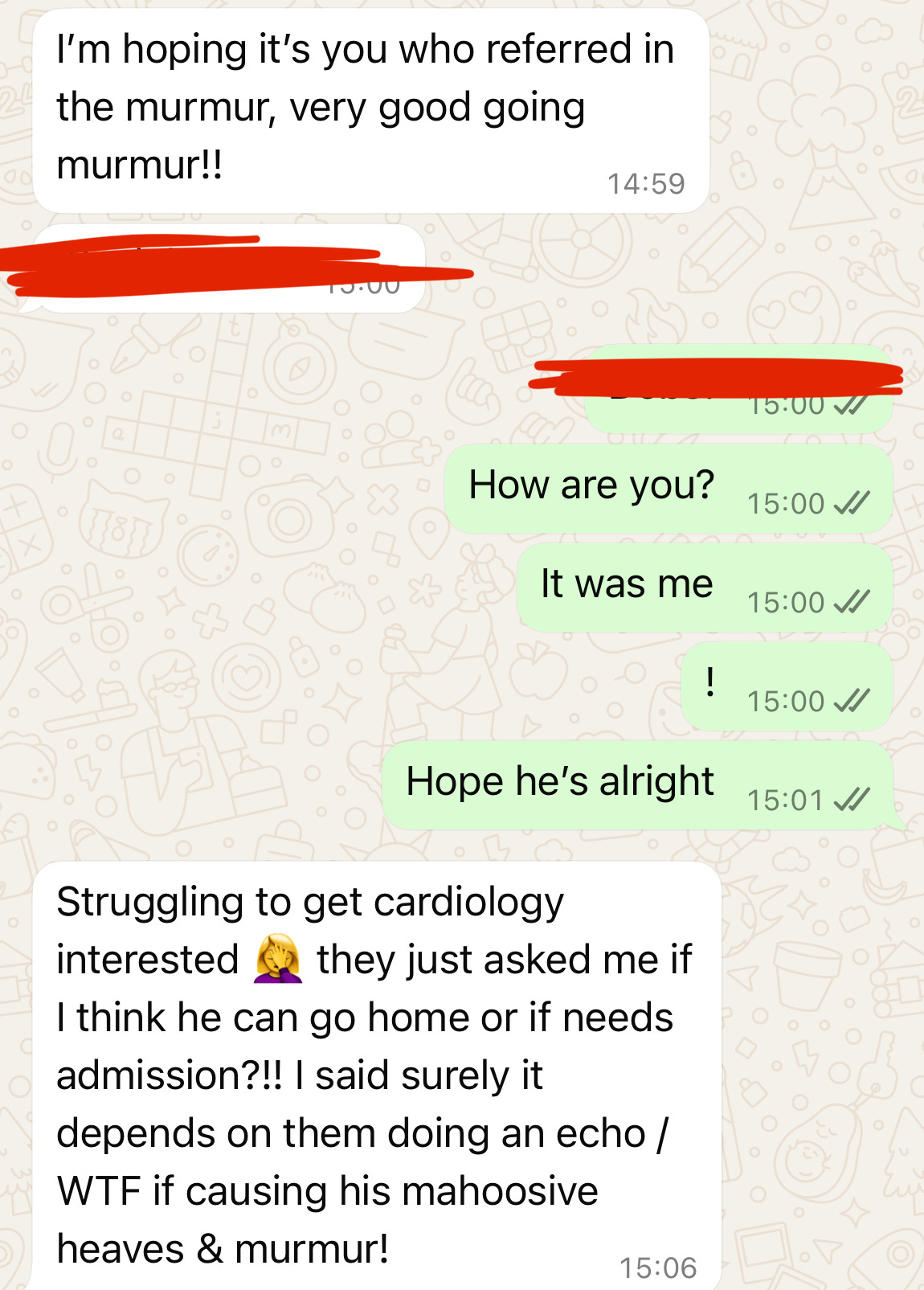
Slightly unhinged response for sure but cardiology were playing hard to get. “Mahoosive” is certainly the right word for this chaps murmur. The conversation continued and it turns out that he became sicker and sicker. He became more short of breath and remained tachycardia.
Life goes on I guess. I went home to a nice meal to open my fast and was back into work the next few days. At the end of the week I received a letter to file from the hospital. It turns out this patient was discharged but the findings were interesting.
He was admitted under cardiology and had a formal echocardiogram which showed:
Severe mitral regurgitation
Right sided and left sided heart failure
Ejection fraction 38%
The cause of this significant deterioration in cardiac function was unknown. There were no vegetations, no signs of an MI and no liver or kidney impairment. He was discharged with a number of diuretics and antihypertensives and was due to be invited to outpatient cardiology for further follow up.
What I’ve Learnt
General practice is tough.
The volume of patients we see is NOT easy and with only 10-15 minutes with each patients, it can be tempting to cut corners. I could have easily thought of this patient as others who have palpitations, but something within me went the extra mile. Going with your gut is important, as your gut is a reflection of previous encounters, observations and experiences.
Recognising murmurs is a crucial skill—it’s a refined art that, like most aspects of medicine, requires a keen ear and practice. I highly recommend investing in a high-quality stethoscope, such as the Littmann Cardiology stethoscope. While electronic stethoscopes aren’t necessary, a cardiology-grade stethoscope features a larger bell, allowing for deeper and more precise auscultation. If you also need a reminder as to how murmurs sound, then I would also suggest videos like this which demonstrate the sound of an ejection systolic murmur.
Hope that was an interesting case for you all. Until next time!
We’re Bringing You CPD from the Experts
This newsletter is mailed out to approximately 4000 clinicians every week and this is only possible because of your support. We’ve always tried to provide high quality content whether that’s our weekly webinars, this newsletter or YouTube videos. We’ve been speaking to lots of clinicians who are in regular contact with our content and it’s clear that many clinicians are looking for some more **SPECIFIC** content. We’re planning sessions on tricky topics like spirometry as well some paediatric focussed content.
As part of this evolution, we’re also bringing in the specialists. Senior registrars and consultants who have detailed insights into crucial topics in medicine and surgery. For example, our next masterclass on CPD Mental Health will be delivered by Dr Michael Case-Upton, senior registrar in psychiatry. Much of mental health management falls on primary and secondary and we’re hoping he can educate us on how to provide the best care in our settings, as well as when we should think about a referral. The topics covered include:
Depression and anxiety including diagnosis and long term management
Schizophrenia: outpatient vs inpatient management and ongoing monitoring
Drugs in psychiatry – SSRIs, antipsychotics, TCAs and more
Mental Health Sectioning and ethical considerations
ADHD diagnosis and management
As part of this webinar you will receive:
3 CPD points (externally accredited)
60 days recorded access
Information about the speaker:
Dr Michael Case-Upton BSc(Hons) MBChB MRCPsych Higher Trainee (ST6) in Forensic Psychiatry
Dr Case-Upton graduated from Sheffield medical school in 2017. He became a Member of the Royal College of Psychiatrists in 2021 having undertaken core psychiatric training in Leeds. He has prior experience of working in community mental health teams and inpatient psychiatric settings. He is currently in his final year of sub-specialty training in Forensic Psychiatry at the Yorkshire Centre for Forensic Psychiatry in Wakefield. His clinical role involves the assessment and treatment of mentally disordered offenders in secure hospitals and prisons, and providing expert psychiatric evidence to the criminal Courts.

Website: www.paretoeducation.co.uk
Instagram: www.instagram.com/pareto_ed
Twitter: www.twitter.com/pareto_ed
Youtube: https://bit.ly/3DPm23c
Email: info@paretoeducation.co.uk