


Pharmacy Closures - Is Pharmacy First a lifeline?
Community Pharmacy in Crisis

It’s been several months since Pharmacy First has launched in the UK and I think I’m seeing the same number of UTIs as I did previously. Of course, this is completely anecdotal so I thought I’d ask a pharmacist I met randomly at a coffee shop about his experiences with pharmacy first.

He confirmed a few things for. His pharmacy continued to dispense lots of medications but didn’t see many patients as part of Pharmacy First. He’s also a well connected chap and told me that this was an experience that pharmacies all around the country were having.
Now hold on a second… I thought this was all about driving demand away from GP practices? It’s clear that it’s not having the intended effects so far so this weeks newsletter is about why Pharmacy First is not quite the “first” choice for patients.
Pharmacies in crisis
This is no understatement. The Guardian has recently reported that 436 community pharmacies closed permanently in 2023, with an additional 13,863 temporary closures in the same year. The number is staggeringly high and it means that patients living in rural or deprived areas are finding it difficult to access a pharmacy. So why are so many pharmacies closing down?
The answer is in how pharmacists get paid. Traditionally, pharmacies used to get paid in threeways:
Dispensing Fees: The NHS pays community pharmacies a fee for dispensing prescription medications to patients. These fees are based on the number of prescriptions processed and the type of medication dispensed. The fee is around £1.29 per prescription item,
Reimbursement for Drugs: Pharmacies are reimbursed for the cost of the drugs they provide. The reimbursement rate is based on the NHS Drug Tariff, which sets the price the government will pay for different medications.
Profit on reimbursement: The NHS reimburses pharmacies based on the drug tariff. Some pharmacies can negotiate better deals to obtain medications at a lower cost. The difference between the lower cost and the reimbursement value can be claimed as profit.
So this means that pharmacies connected to GP practices, nursing homes, care homes, clinics such as STI clinics managed to do very well. The more patients that came to them, the more money they made. This effect was enhanced when out of hours services really took off in the UK.
Pharmacists started to become “24-hour pharmacies” and managed to get more prescriptions on their books. As you can see, those pharmacists associated with GP practices and based in urban, well-populated areas were at a significant advantage.
However, this push in dispensing started to take away from the joys of community pharmacy. You see, community pharmacy has a similar appeal to general practice. Pharmacists can get to know patients, appreciate the long term needs of patients and work with GPs to maximise care for patients. Historically, community pharmacists would even meet GPs and nurses to discuss cases. This rarely happens now. This means pharmacists have opted to move either into secondary care or more recently, primary care where there is greater scope for patient care and clinical problem solving.
It is all these factors that have caused pharmacies to struggle. Funding is geared towards urban, highly populated pharmacies and pharmacists have opted to shift to other settings.
Why is Pharmacy First a lifeline?
As much as this is about patient care, Pharmacy First is also about resuscitating community pharmacy. Over the years, pharmacists have been asked to become more “clinical” and have had certain extended services commissioned.
This has included seeing and treating minor ailments, contraception counselling and diagnosing and managing hypertension. Pharmacies are paid for these additional services and for community pharmacists, it re-injects them with the ability to problem-solve. This has also been aided by the creation of the pharmacy technician role who are incredibly helpful in taking over some of the dispensing related tasks from pharmacists. The final checks are in the hands of pharmacists of course, but it frees the pharmacist to perform more varied roles.
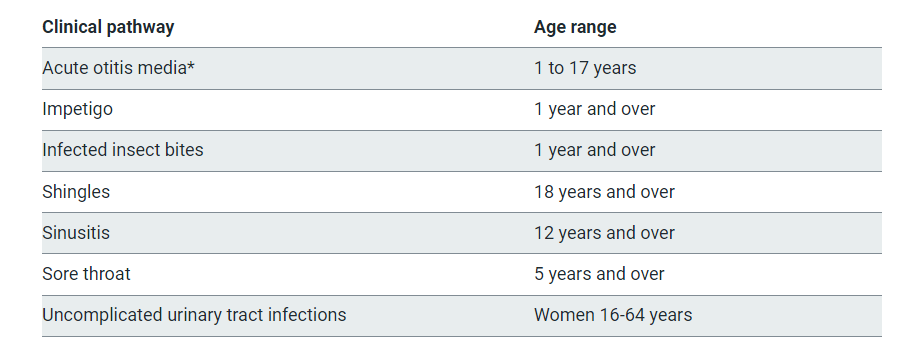
Pharmacy First is an extension of this. Each consultation is paid at £14 with an additional £1000 for the achievement of certain targets patient targets. Pharmacists throughout the country are asked to upskill in order to consult and treat common infections (shown in image below). Additionally, MPharm undergraduate courses have all started to incorporate a clinical skills component into the degree with the NHS providing a further financial incentive to those wanting to become an independent prescriber (IP). This is in order to expand the scope of pharmacists to assess and treat patients.
Why We Should Support Pharmacists
In the proper MDT spirit that Pareto Education advocates for, we believe pharmacists bring an incredible skillset to the fabric of our workforce. Their ability to understand the mechanism of medications, rationalise them and ensure their safe dispensing makes them a limb the NHS cannot function without.
Pharmacists are trying their best to upskill with regards to clinical diagnosis and examination. It might be easy for us to grab an otoscope to examine an ear, check the ear drum and appreciate the signs of otitis media but it certainly is not easy for pharmacists. They are having to climb a mountain to provide these services and here are some ways in which we can assist them:
If you have a pharmacy in your hospital or attached to your practice, offer to do some teaching on clinical history taking, examination and management. It will help your colleagues and get you some ticks on your portfolio!
Make sure you actively signpost patients who come in for common conditions. We all have that “repeated UTIs with normal investigations.” Next time they have dysuria or frequency, they could always go to their local pharmacy!
Don’t be upset if a pharmacist bounces a patient back! Our colleagues are junior in their experiences in comprehensively assessing patients and are learning on the go. Try and reach out to them and give them some feedback.
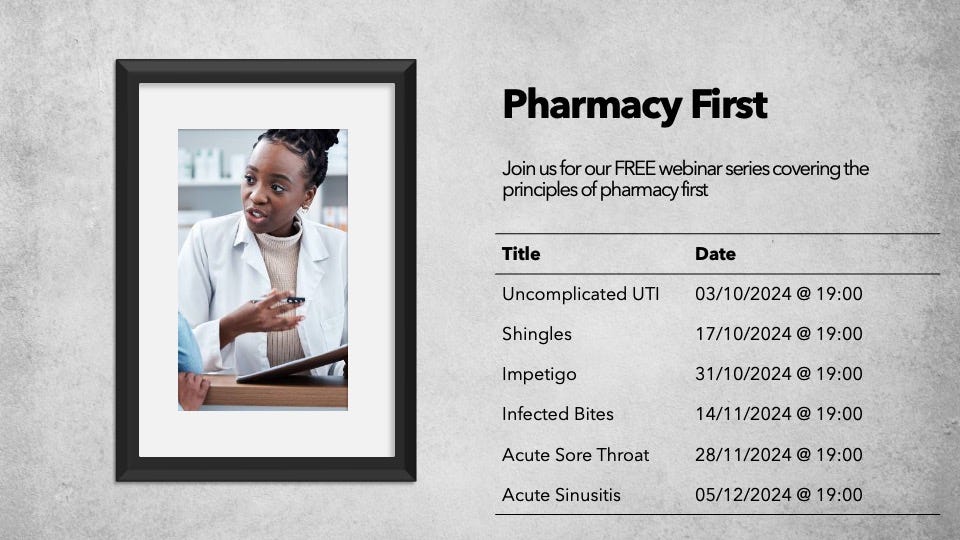
We at Pareto Education are trying our best to support community pharmacists by running a FREE Pharmacy First webinar series. We would be grateful if you could spread the word to your colleagues. They are free to access, held online and act as an opportunity for pharmacists to obtain some clarity on clinical topics. I’ve put the poster below so feel free to share it! Here’s the link
Until next time..
Qualified Professional? Check out our FREE webinars!
At Pareto, we’re all about feedback and we’ve reflected on some of our events. We realised that our followers who are qualified professionals tend to request teaching on clinical scenarios, disease and management. In light of this, we’ve defined a fantastic list of FREE webinars for qualified professionals covering some tricky, but common presentations. These include:
Tired all the time
Managing pyrexia in children
Rashes 101
Substance Misuse
Headaches
These are FREE, held online and form an opportunity to re-fresh or learn new principles relating to common presentations. Don’t delay and sign up here.
Until next time!
Check us out on our various pages
Website: www.paretoeducation.co.uk
Instagram: www.instagram.com/pareto_ed
Twitter: www.twitter.com/pareto_ed
Youtube: https://bit.ly/3DPm23c
Email: info@paretoeducation.co.uk